Wegovy pill from $149/month
The FDA-approved weight loss pill is here
No injections. Just once-daily Wegovy® with proven results—up to 17% average weight loss in trials.

Can Zepbound help with weight loss? Yes — when paired with healthy habits, Zepbound (tirzepatide) can lead to meaningful, sustained weight loss for many adults with obesity or overweight and a related health condition. The FDA first approved Zepbound in 2023 for chronic weight management, and in 2024 it also gained approval to treat moderate to severe obstructive sleep apnea (OSA) in adults with obesity. We’ll cover how it works, how effective it is, side effects, dosing, costs and coverage, and safe alternatives — so you can decide, with your clinician, if it fits your plan.
GLP-1 dosing follows a predictable titration pattern—see our complete guide to GLP-1 dosing schedules to understand what to expect.
GLP-1 medications share a similar side effect profile. Our breakdown of GLP-1 side effects and when to call your doctor applies to Zepbound as well.
Zepbound is the brand name for tirzepatide, a once-weekly injection that activates two gut-hormone receptors — GLP-1 and GIP — to reduce appetite and food intake. It’s part of a newer class of medications for chronic weight management and is also approved to treat moderate to severe OSA in adults with obesity. It should always be used alongside a reduced-calorie diet and increased physical activity. It is not known to be safe or effective in children.
Yes. The FDA approved Zepbound on November 8, 2023, for chronic weight management in adults with a BMI ≥30, or ≥27 with at least one weight-related condition (such as high blood pressure, type 2 diabetes, or high cholesterol). That means Zepbound is not an “off-label” choice for weight loss — it’s on-label. (Its sister brand, Mounjaro, contains the same active ingredient but is approved for type 2 diabetes.) Insurance coverage still varies widely by plan.
Zepbound mimics two incretin hormones — GLP-1 and GIP — that help regulate hunger, fullness, and how quickly food empties from your stomach. By activating these receptors, tirzepatide lowers appetite and reduces food intake. Many patients notice they feel full sooner, think about food less, and tolerate smaller portions. Because the medicine slows stomach emptying, doctors raise the dose gradually to reduce gastrointestinal (GI) side effects. As the FDA explains, Zepbound is given once weekly and escalated over several weeks to a maintenance dose.
“Obesity and overweight are serious conditions … (Zepbound's FDA approval) addresses an unmet medical need,” says John Sharretts, MD, an FDA division director, underscoring that medications like tirzepatide target biology, not willpower.
In the pivotal SURMOUNT-1 trial (adults with obesity/overweight without diabetes), participants taking tirzepatide plus lifestyle changes lost on average about 15% of body weight at 5 mg, 19.5% at 10 mg, and 20.9% at 15 mg over 72 weeks—versus ~3% with lifestyle plus placebo. More than half on higher doses achieved ≥20% weight loss.
Head-to-head data also matter. In SURMOUNT-5, an open-label trial in adults with obesity without diabetes, tirzepatide led to greater average weight loss at 72 weeks than semaglutide (−20.2% vs −13.7%), and more people reached deeper weight-loss thresholds (≥10%, ≥15%, ≥20%, ≥25%).
“Medications work best with healthy habits, but for many patients, tirzepatide delivers weight loss on par with what we once expected only from surgery,” notes Cecilia Low Wang, MD, endocrinologist at the University of Colorado.
Zepbound is indicated for adults with a BMI ≥30, or ≥27 with at least one weight-related condition (for example, high blood pressure, type 2 diabetes, high cholesterol, OSA). It is not approved for children. Older adults can use it; no specific dose adjustment is recommended solely for age, though tolerability should guide dosing.
Who should avoid it? People with a personal or family history of medullary thyroid carcinoma (MTC) or Multiple Endocrine Neoplasia syndrome type 2 (MEN2) should not take Zepbound. It hasn’t been studied in those with severe GI disease (including severe gastroparesis), and clinicians use caution in patients with a history of pancreatitis. Zepbound should not be used with other tirzepatide products or GLP-1 receptor agonists. If you’re pregnant, planning pregnancy, or breastfeeding, talk with your clinician; the label advises stopping Zepbound when pregnancy is recognized.
Common side effects include nausea, diarrhea, vomiting, constipation, abdominal pain/indigestion, injection-site reactions, fatigue, burping, hair loss, and reflux. These often occur during dose increases and may improve over time.
Less common but important risks have been observed with this class, including gallbladder problems (such as gallstones or cholecystitis), kidney injury (often related to dehydration from vomiting/diarrhea), and inflammation of the pancreas (pancreatitis). Zepbound can worsen diabetic retinopathy in people with diabetes, and it carries warnings about depression or suicidal thoughts. Because it slows stomach emptying, there’s also a precaution about pulmonary aspiration during anesthesia or deep sedation; tell your surgical and anesthesia teams you’re taking it.
Safety tips that help many patients: escalate slowly as prescribed; favor smaller, protein-forward meals; limit high-fat foods (which can worsen nausea); and stay well-hydrated to reduce dehydration-related risks. If severe stomach pain occurs (especially with vomiting), or if mood changes or vision changes appear, call your clinician promptly.
“Patients should let us know about any planned procedures,” says Sally Seymour, MD, an FDA division director, noting aspiration has been reported in people on GLP-1-type medicines undergoing anesthesia.
You’ll start at 2.5 mg once weekly for 4 weeks, then increase by 2.5 mg every ≥4 weeks as tolerated. For weight reduction/maintenance, the usual maintenance dose is 5 mg, 10 mg, or 15 mg weekly (maximum 15 mg). For OSA, the maintenance dose is 10 mg or 15 mg weekly. If you miss a dose, take it as soon as possible within 4 days (96 hours); otherwise, skip and take your next dose on the usual day. Do not “double up.”
“Slow, steady titration is key — it allows the gut to adapt and minimizes side effects,” adds Dr. Low Wang.
Expect appetite to return and weight to creep back without a plan. In a randomized withdrawal study (SURMOUNT-4), participants who switched from tirzepatide to placebo after significant weight loss regained weight, while those who continued treatment maintained or lost more. This pattern — plateau on therapy, regain off therapy — mirrors what we see with other obesity medicines. Long-term weight maintenance hinges on ongoing treatment and strong lifestyle routines.
Because Zepbound is already FDA-approved for chronic weight management, off-label use is less relevant here. Clinicians may still prescribe “off-label” in specific circumstances (for example, patients slightly outside labeled criteria), but coverage is often harder to secure and requires prior authorization. Regular follow-up for dose adjustments, side-effect management, and nutrition/exercise support remains essential for safety and results.
Use caution. The FDA has warned about unapproved or compounded “GLP-1” products sold online, including products labeled as semaglutide or tirzepatide. Some have contained different chemical forms (e.g., salt forms) that are not the same as the approved drugs, or have led to dosing errors and adverse events. Compounded drugs should be used only when an FDA-approved product is on shortage and a prescriber determines it’s clinically necessary. If you must use a compounded medication, verify the pharmacy is state-licensed (and for 503B outsourcing facilities, FDA-registered).
Cash prices are high; list prices for this class are roughly around $1,000 per month, though your out-of-pocket costs depend on insurance and discounts. Coverage for obesity medications varies: many employer plans require prior authorization or step therapy, Marketplace plan coverage remains limited, and Medicare coverage has been evolving via proposals and policy changes. Coverage may be more straightforward for diabetes, and some plans may cover Zepbound for OSA. Ask your insurer about criteria and documentation needed.
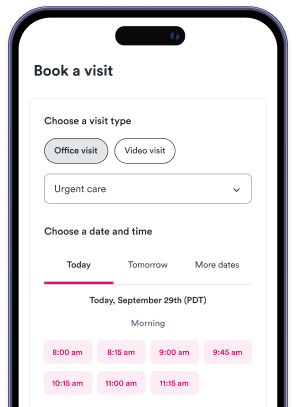
Finding care fast: If you don’t have a primary care clinician or endocrinologist, you can book same-day primary care or urgent care through Solv, or use Solv to find telemedicine visits for medication management and side-effect troubleshooting.
Medication works best with simple, sustainable habits:
Protein and fiber: Aim for protein at each meal and fiber-rich foods (most adults need ~22–34 grams/day) to promote fullness. Increase fiber gradually and drink water.
Resistance training: Two or more days/week of muscle-strengthening activities helps preserve lean mass as you lose weight. Add at least 150 minutes/week of moderate activity, if you can.
Hydration and sleep: Fluids help limit dehydration from GI side effects; consistent sleep supports weight management.
“These medicines aren’t a replacement for healthy living — think of them as a tool that works best with nutrition, movement, and sleep,” says Dr. Low Wang.
Other GLP-1/GIP options: Semaglutide (Wegovy) is FDA-approved for weight management and remains a strong alternative; dose is titrated to a 2.4 mg weekly injection for most indications. An oral semaglutide pill is now available in 2026. Head-to-head data suggest tirzepatide leads to greater average weight loss, but both are effective.
Non-GLP-1 medications: Depending on your health profile, options include phentermine/topiramate ER, bupropion/naltrexone ER, and orlistat — each with unique benefits and side effects. Discuss fit and contraindications with your clinician.
Bariatric surgery: For higher BMIs or obesity-related complications, surgery can produce 25–30% or more long-term weight loss, but it’s invasive and requires lifelong follow-up.
Lifestyle-only approach: Nutrition, physical activity, sleep, and stress management remain foundational — especially for people not ready for medication or surgery.
Start with your clinician. Primary care, obesity medicine, or endocrinology can review your history, goals, meds, and labs (often A1c, fasting lipids, kidney function) and discuss risks/benefits. You can use Solv to find nearby primary care or schedule a telemedicine visit to discuss options.
Plan follow-up. Early check-ins during titration help fine-tune dosing and manage side effects.
Coordinate care. Tell your dental/surgery teams you’re on tirzepatide; ask about pre-procedure guidance. Bring up pregnancy plans and contraception—tirzepatide can lower the effectiveness of oral birth control during the first 4 weeks after starting and after each dose increase, so use a non-oral or add a barrier method for those 4 weeks.
FDA-approved for chronic weight management in adults; also approved for OSA with obesity.
Average weight loss reached ~15–21% at 72 weeks in trials.
Common side effects are GI; slow titration and hydration help.
Stopping often leads to weight regain; plan for maintenance.
Coverage varies widely; expect prior authorization.
Deciding between medications? Our comparison of injectable versus oral GLP-1 options can help you have a more informed conversation with your prescriber.
Zepbound is the brand name for tirzepatide, a once-weekly injection that activates two gut-hormone receptors—GLP-1 and GIP—to reduce appetite and food intake. It is part of a newer class of medications for chronic weight management and is also approved to treat moderate to severe obstructive sleep apnea (OSA) in adults with obesity. It should always be used alongside a reduced-calorie diet and increased physical activity.
Yes, Zepbound was approved by the FDA on November 8, 2023, for chronic weight management in adults with a BMI ≥30, or ≥27 with at least one weight-related condition such as high blood pressure, type 2 diabetes, or high cholesterol.
People with a personal or family history of medullary thyroid carcinoma (MTC) or Multiple Endocrine Neoplasia syndrome type 2 (MEN2) should not take Zepbound. It hasn’t been studied in those with severe GI disease, and clinicians use caution in patients with a history of pancreatitis. Zepbound should not be used with other tirzepatide products or GLP-1 receptor agonists. If you’re pregnant, planning pregnancy, or breastfeeding, you should consult with your clinician.
Common side effects include nausea, diarrhea, vomiting, constipation, abdominal pain/indigestion, injection-site reactions, fatigue, burping, hair loss, and reflux. Less common but important risks include gallbladder problems, kidney injury, and inflammation of the pancreas. Zepbound can worsen diabetic retinopathy in people with diabetes, and it carries warnings about depression or suicidal thoughts.
If you stop taking Zepbound, you can expect your appetite to return and your weight to gradually increase without a maintenance plan. Long-term weight maintenance hinges on ongoing treatment and strong lifestyle routines.
No. Do not combine Zepbound with other tirzepatide products (like Mounjaro) or with any GLP-1 receptor agonist. Doing so may raise risks without added benefit.
No injections. Just once-daily Wegovy® with proven results—up to 17% average weight loss in trials.

Dr. Linda Halbrook is a Board-Certified Family Medicine physician with over 40 years of experience, dedicated to providing comprehensive care to patients across Texas. She retired from practice but currently serves on the Clinical Services Committee of CommonGood Medical, a non-profit organization serving the uninsured in Collin County.
Medically reviewed
View this article's sources and history, and read more about Solv's Content Mission Statement, editorial process, and editorial team.
Solv has strict sourcing guidelines and relies on peer-reviewed studies, academic research institutions, and medical associations. We avoid using tertiary references.
Solv’s team of medical writers and experts review and update our articles when new information becomes available.
Written by Solv Editorial Team
Medically reviewed by: Dr. Rob Rohatsch, MD
Edited by Solv Editorial Team
Medically reviewed by: Linda S. Halbrook, MD
Edited by Solv Editorial Team
Edited by Solv Editorial Team
Edited by Solv Editorial Team
Edited by Solv Editorial Team
Edited by Solv Editorial Team
Edited by Solv Editorial Team
Edited by Solv Editorial Team
No injections. Just once-daily Wegovy® with proven results—up to 17% average weight loss in trials.